














Aspadol 200 mg: Powerful Relief for Severe Pain – Complete Patient Guide
Explore Aspadol 200 mg (tapentadol): how it works, recommended uses, dosage guidance, side effects, warnings, and safe-use tips in this full-length patient guide.
1. Introduction
Severe painduetomajor surgery, cancer,debilitatingchronicdisease, or traumatic injurycallsfor powerful,trustworthymedication. Aspadol 200?mg,whichincludestapentadol,presentsanintriguingalternative. Its dual mechanismopioidactivityplusnorepinephrine reuptake inhibitioniseffective for both nociceptive and neuropathic pain. Thishandbooksummarizesallyou need to know: how it works, whento useit, dosage and administration,advantages,dangers, andoptimumsafetymeasures.
2. What Is Aspadol 200?mg and How Does It Work?
Aspadol (tapentadol) is a centrally acting analgesic with a two-pronged mechanism:
-
Mu-opioid receptor agonism dampening ascending pain signals in the brain and spinal cord.
-
Norepinephrine reuptake inhibition (NRI) enhancing descending inhibitory pain pathways.
Bycombiningthesemechanisms,Aspadolcanaddressawidercategoryof pain typesincluding severe musculoskeletal pain, cancerpain, and neuropathic painpotentially reducingfrequentopioid side effects.
3. Approved Uses & Pain Conditions
Aspadol 200?mg (usuallyin extended-releaseformulation) isusedwhenintense,round-the-clock painreliefisrequired. Approved usesare:
-
Severe acute pain (e.g., post-surgical or traumatic)
-
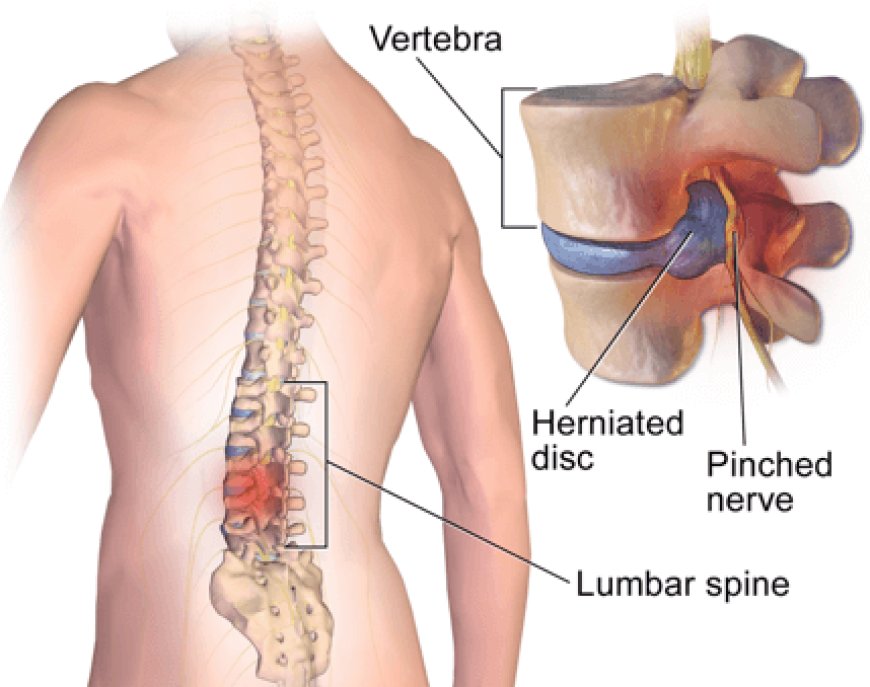
Chronic musculoskeletal pain (e.g., severe arthritis, back pain)
-
Cancer-related pain
-
Neuropathic pain (e.g., diabetic neuropathy)
Its reserved for cases where milder painkillers are insufficient and in line with clinical guidelines.
4. Clinical Efficacy: What the Research Shows
4.1 Acute Post-Surgical Pain
Researchindicatesthat a singledose of200?mgtapentadolprovidesanalgesiaequivalenttothat of60?mg morphinebuthasfewer gastrointestinalcomplaints.
4.2 Chronic Musculoskeletal & Neuropathic Pain
OsteoarthritisandneuropathypatientsinPhaseIIIstudiesindicatedthattapentadol ER (100250?mg BID)isas effective asoxycodone in painbutbetter tolerated,especiallywithregardto gastrointestinalside effects.
4.3 Real-World Patient Testimonials
Dozensof patient reportsreportgood12-hour painreliefandlessdosetitrationrelatedto side effectsalthough someneedindividualizeddosingbecauseofdizziness or nausea.
5. Why Choose the 200?mg Dose?
The 200?mg dose (ER formulation) often marks the mid or upper-therapeutic range. At this level:
-
Dual mechanism provides steady opioid and NRI action.
-
Supports pain relief for up to 12 hours, suiting long-term use for chronic conditions.
-
Provides a consistent analgesic effect ideal for scheduled dosing.
6. Safe & Effective Dosage Guidelines
Starting Dose
-
50?mg ER BID for opioid-nave individuals; increase based on pain control.
Typical Range
-
100250?mg ER BID, max 500?mg/day. IR tablet may be used sparingly for breakthrough pain, but total dose across all forms must not exceed safe limits.
Administration
-
Swallow tablets whole, with water. Avoid crushing or chewing to prevent overdose.
Titration & Monitoring
-
Increase slowly, evaluating pain relief and side effects every few days.
-
Begin monitoring for respiratory depression and dizziness, especially within the first 72 hours or after dose increases.
7. Benefits Compared to Other Opioids
| Feature | Aspadol 200?mg (Tapentadol ER) | Traditional Opioids (Morphine/Oxycodone) |
|---|---|---|
| Neuropathic Pain | Dual mechanism helps | Limited effect |
| Constipation & Nausea | Lower incidence | High incidence |
| Dosing Frequency | 12-hour intervals | 46 hours |
| Abuse Risk | Moderate | High |
| CYP Interactions | Minimal | Significant |
Aspadol 200 mg provides balanced pain relief with improved tolerability and fewer drugdrug interactions.
8. Common Side Effects & Management
According to health sources like HealthDirect and Drugs.com, common side effects include:
-
Constipation Manage with fiber, fluids, and laxatives.
-
Drowsiness/dizziness Avoid driving/machinery until tolerance builds.
-
Nausea/vomiting Take with food; use anti-emetics if needed.
-
Headache, dry mouth, sweating Monitor and address symptomatically.
If side effects persist, consult your healthcare providerdosage adjustments may be needed.
9. Serious Risks & Warnings
Aspadol carries significant risks, including:
Respiratory Depression
Risk isgreatestbetween2472 hours ofdoseincreaseortreatmentinitiation,particularlywhenconcomitantlyadministeredwith othercentralnervous systemdepressants.
Addiction & Misuse
As a Schedule II opioid, tapentadolmaycausemisuse, addiction, or overdose, even attherapeuticdoses. REMSprogramsnecessitateprovider and patient education.
Serotonin Syndrome
Concurrent use with SSRIs, SNRIs, triptans, or MAOIs may trigger serotonin syndrome.
Seizure Risk
Tapentadol may lower seizure thresholdsuse with caution in at-risk patients.
Hypotension & Adrenal Suppression
Standing too quickly may cause dizziness and fainting; long-term use may suppress adrenal function.
Pregnancy/Newborn Withdrawal
Chronic maternal use may cause neonatal withdrawal syndrome.
10. Precautions & Drug Interactions
Do not use Aspadol if you have:
-
Acute/severe asthma or COPD
-
Bowel obstruction (e.g., paralytic ileus)
-
Taken MAO inhibitors within the past 14 days
Be cautious with:
-
Alcohol, benzodiazepines, other opioids due to sedation and respiratory risk.
-
SSRIs/SNRIs, triptans, serotonergic agents due to serotonin syndrome risk.
-
Seizure-prone patients due to lowered threshold.
Consult your doctor/pharmacist before combining with supplements or other medications.
11. Use in Special Populations
-
Older adults are more susceptible to sedation, respiratory depression, and hypotensionstart low and monitor closely.
-
Pregnancy/Breastfeeding: Only when absolutely necessarymonitor neonates for withdrawal.
-
Liver/Kidney impairment: Dose adjustments and monitoring required.
12. Safe Discontinuation & Withdrawal Management
Long-term use can lead to physical dependence. To prevent withdrawal:
-
Taper gradually (e.g., 1025% dose reduction weekly) under medical supervision.
-
Monitor for cravings, mood changes, sweating, etc.
-
Provide support: medication-assisted therapy or counseling if needed.
Never stop abruptlywithdrawal can include serious symptoms like tremors, anxiety, vomiting, and insomnia.
13. Monitoring & Patient Education
Healthcare providers should:
-
Conduct ongoing REMS counselingsafe use, storage, and disposal of medication .
-
Encourage patients to store securely, avoid sharing, and track doses.
-
Monitor for signs of addiction or respiratory issues, especially during the first weeks.
14. Responsible Use & Alternatives
Aspadol 200?mg is best used when:
-
Pain is severe, chronic, or neuropathic and unresponsive to non-opioid options.
-
Not the first choice for mild-to-moderate painconsider NSAIDs, acetaminophen, or neuromodulators.
-
Short-term opioid use is preferred when possible.
Always integrate non-drug strategies: physical therapy, CBT, weight control, and other pain management modalities.
15. Abuse & Misuse Trends A Public Health Perspective
Currentmediareportsemphasizeincreasingtrendsof tapentadolmisusesuchasillicit injection and onlinecounterfeitinginIndiaandother countries.Suchpracticeshaveresultedinseveremedicalrepercussionssuchasclots and infections,necessitatingcloserregulationand enforcement.
Thishighlightstheneedforobservationandprotectionagainst medication diversion orabuse.
16. Quick FAQ
Q: How quickly does Aspadol work?
A: ER peaks in about 68 hours and provides relief for 12 hours; analgesic effect begins ~1 hour after dose.
Q: Can I drive while taking it?
A: Avoid driving until you know how you respond; drowsiness/dizziness are common early on.
Q: Is it addictive?
A: YesSchedule II opioids have high addiction potential; use as prescribed with monitoring.
Q: What about breastfeeding?
A: Use with extreme cautionnippling infants may experience respiratory depression.
Q: Can I drink alcohol on Aspadol?
A: Neveralcohol significantly increases risk of overdose.
17. Final Takeaway
Aspadol 200?mgprovidesintense, long-lasting relief forbad, mixed-type paindueto its dualaction.Incontrasttoclassicalopioids, itprovideseffective painreliefwithdecreasedgastrointestinal effects and fewer drug interactions,yetstillposesserious risks thatrequireappropriateuse.